
Starting an HIV Prevention Revolution with Test and Treat
Foreword: Lancet Chief Editor Richard Horton recently twitted (16 April 2011) that in the 19th century “the pamphlet was a means to ignite new thinking” adding, “Is there a place for the pamphlet today? Even in medicine and public health?” This is a question I often asked myself particularly in the field of HIV which is very much sensitive to what can be said, by whom and how. The following was written before Horton’s twit and was turned down for publication by The Lancet. A stand too far?
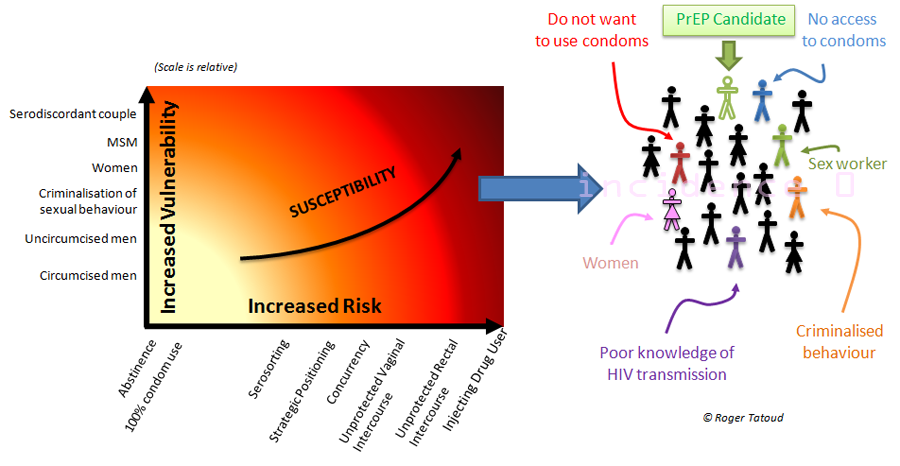
 HIV prevention as we know it and have done it for the last 30 years is failing to put an end to the HIV epidemic. At best current prevention strategies appear to be containing HIV incidence to a rate of 2.6 million new infections a year after a peak at 3.5 million in 1996 (1). The recent acknowledgment that there is more to HIV prevention than the ABC of behaviour change and condoms and that key vulnerable populations have been largely ignored by prevention interventions (injecting drug users, men who have sex with men) is a welcome but late awakening. Nevertheless, thirty years into the epidemic and in the absence of a cure or any other means to protect oneself, there are still men and women who cannot or will not use condoms in situations where they are at risk of being infected. Their reasons are multiple, complex and often beyond human rational decision making or control (2). In trying to address each of them, often in turn, independently and above all within the narrow epidemiological context of HIV, attempts at preventing new HIV infections have resulted in limited outcomes and the fragmentation of the scarce resources allocated to target an epidemic of global extent and ramifications.
HIV prevention as we know it and have done it for the last 30 years is failing to put an end to the HIV epidemic. At best current prevention strategies appear to be containing HIV incidence to a rate of 2.6 million new infections a year after a peak at 3.5 million in 1996 (1). The recent acknowledgment that there is more to HIV prevention than the ABC of behaviour change and condoms and that key vulnerable populations have been largely ignored by prevention interventions (injecting drug users, men who have sex with men) is a welcome but late awakening. Nevertheless, thirty years into the epidemic and in the absence of a cure or any other means to protect oneself, there are still men and women who cannot or will not use condoms in situations where they are at risk of being infected. Their reasons are multiple, complex and often beyond human rational decision making or control (2). In trying to address each of them, often in turn, independently and above all within the narrow epidemiological context of HIV, attempts at preventing new HIV infections have resulted in limited outcomes and the fragmentation of the scarce resources allocated to target an epidemic of global extent and ramifications.
To date, of the prevention interventions tested in clinical trials, only four have shown a positive outcome: male circumcision, a complex and costly combination vaccine, and two approaches based on HIV-uninfected people being given anti-retroviral drugs (aka pre-exposure prophylaxis) whose efficacy hinges on adherence (3-5). Although these trials showed encouraging results, there are multiple challenges to effectively deliver these interventions on the scale necessary to observe a significant and rapid reduction in HIV prevalence at a population level. The result of the CAPRISA 004 tenofovir vaginal microbicide trial may have well called for a rethink of the field of HIV prevention as Ward Cates proposed (6), yet a change in the prevention lexicon will be a small step towards population level elimination of HIV transmission. Optimism based on mathematical models predicting that these interventions could prevent millions of new infections and death in the next two decades should be tempered by the millions who will still become infected and die at current rates of infection and death. Furthermore there are ethical considerations in developing an approach employing antiretroviral therapies for people not infected with HIV, whilst there are still insufficient drugs available for the 10 million people living with HIV and AIDS in need of life saving treatment.
Conversely, there are growing evidences that a different approach to HIV prevention could offer the long sought after answer to the growing problem of providing universal access to ARV (7, 8). Indeed, for every two HIV infected people starting treatment, five are infected. At the current rate of infection the cost towards achieving and maintaining universal access is spiralling out of control rising to US$42 billion in 2010, and US$54 billion by 2015, and bearing in mind current funders’ commitment, is not sustainable.
Test and Treat to the rescue?
This controversial approach known as Test and Treat (also known as Universal Test and Treat or Treatment as Prevention) proposes the introduction of universal testing followed by immediate treatment of all those infected regardless of CD4 count and symptoms. The approach is neither recent (9) nor specific to the prevention of HIV (e.g. DOTS for tuberculosis) and has been presented, reviewed and discussed time and again (10-15). It has gain momentum since a seminal article published in The Lancet in 2009 by Reuben Granich and collaborators (16).
A key premise of the Test and Treat approach is that everybody should first be able to test for HIV. Doing this successfully means more than just addressing the current obstacles to voluntary counselling and testing (VCT) or extending its current level (17). Stigma and discrimination are key factors affecting VCT and treatment uptake, but the damages caused by the epidemic extend far beyond the individual, affecting entire communities and countries shattering economic and social life, and hindering access and delivery of VCT, treatment and care. For this very reason, a global public health approach targeting the epidemic at the population level needs to be implemented within a development and public health context rather than one of a disease which affects specific groups.
Test and Treat represents an opportunity to eliminate HIV transmission through mainstreaming and embedding HIV prevention in other interventions, in particular development interventions, which together provide an opportunity to repair and rebuild what the epidemic has broken. This is a different approach than that based on individuals being asked to take responsibility for their acts notwithstanding their environment.
 |
| This map shows that in areas where CD4+ cell counts at the time of therapy initiation are known, the majority of geographic locations suffer from late diagnosis, and therapy is consistently initiated at CD4+ cell counts < 200 cells/mm3 (Egger M, et al. CROI 2007. Abstract 62). |
Despite mounting evidences that it could both work (18-20), be cost effective (21), and has individual health benefits (22), opposition to Test and Treat remains fierce amongst researchers, public health authorities, philanthropic and institutional funders, their anxious grant recipients, the polity for which cost matters, and notably amongst advocates and activists (23). Undoubtedly, Test and Treat has been politicised long before being critically examined or even tested, but at a time when a majority or more of those diagnosed with HIV (from Thailand to the UK via Brazil and of course many African countries) need to start treatment at the time of diagnosis, we have already entered the era of Test and Treat.
“We can’t treat ourselves out of the epidemic”, or can we?
The approach presents numerous difficulties, in that it challenges current wisdom and dogma, threatens new promising interventions and research that despite years of investment has failed to deliver. However, Test and Treat should not be pitted against other interventions and none of its difficulties are insurmountable or necessarily costly (since cost can be shared with or spread across other interventions). In the current context of limited financial resources allocation, Test and Treat would require a thorough assessment of current bugdet priorities (not only in the health or research sector). It would require political commitment and acknowledging the existence of population, often marginalised, more susceptible to HIV infections and the necessity to address their needs, not as vulnerable or at-risk populations, but simply because their needs deserve to be addressed like any other member of society.
Test and Treat could be the driver for the mainstreaming of HIV prevention that was identified as an essential approach for expanding multi-sectoral responses to HIV/AIDS (24) but which has failed to materialise. A thoughtfully and thoroughly implemented Test and Treat strategy would be more than just the medicalisation of HIV/AIDS (25) but a capacity building process putting in place the structures that would also benefit other existing (circumcision) or forthcoming interventions (vaccines, PrEP). It would have to address issues of human rights, stigma, discrimination, resources and infrastructures altogether and would be implemented alongside circumcision, condoms and STI treatments.
Test and Treat: a Development Framework
Test and Treat is the perfect example of an extended Combination Prevention approach much touted nowadays as the future model for HIV prevention (26). As such, Test and Treat may well not start by expanding testing level but by building the road that leads to the clinic, staffed by well trained nurses and doctors who are critical to deliver both VCT and treatment. Healthcare workers will be empowered to deliver services in severely resource-constrained settings using approaches in which the need for expensive laboratory tests is reduced (27) and cheaper, reliable point of care technology used to monitor disease progression. Of course, Test and Treat, if it went wrong or wasn’t delivered correctly, could lead to the emergence of drug resistance, human rights coercion, drug supply failure, and increased risk of transmission from people with acute infection or stopping drugs along with their viral rebound. These dangers need to be acknowledged and managed. This is why Test and treat requires honesty, courage and determination and demands leaving aside dogma, moot objections and entrenched positions.
Consequently, beyond basic and clinical research, funding may not always support interventions directly related to HIV. For example, supporting the development of a North South corridor through sub-Saharan Africa to boost regional and international trade (28) may sound remote from HIV prevention but the inclusion of clinics offering testing or treatment and care along a trade corridor that doubles as HIV highway would cost little and contribute significantly to controlling the epidemic. Openly and ardently fighting bills that criminalise homosexuality, if necessary through interventionism as done with development aid, will ensure that men who have sex with men (MSM) are not driven underground any further and have access to the services they need. Ensuring fair access to education for all, boys and girls, will contribute to the training of the next generation of doctors and nurses that are critical to treatment delivery (29), and redress gender imbalance. Many of these interventions are ongoing but they are often disjointed, kept apart in MDG silos, focusing on the individual rather than his environment, distorted by an accountant culture of targets to reach rather than positive impact for individuals; lacking a global impetus, resources and dare I say meaning, they struggle to deliver a rapid and significant impact on the HIV epidemic.
Igniting new thinking?
The field of HIV prevention is at a turning point in its history. The forthcoming results of further trials of New Prevention Technologies and a growing recognition that treatment can also contribute to prevention, all happening on the background of an economic recession are creating confusion and dilemmas amongst advocates, funders and beneficiaries as to what should be done next to successfully contained and quell the HIV epidemic. With the achievements of the Millennium Development Goals being reviewed and a “prevention revolution” at the heart of the next UNAIDS strategic plan for 2011-2015, a bold and global strategy based on Test and Treat could be the starting point for this much needed HIV prevention revolution.
rjt
| Notes:Antiretroviral therapy can be used strategically to reduce the HIV viral load of an HIV-infected individual, and consequently its infectiousness thereby limiting the risk of onward viral transmission. Ideally, Universal Test and Treat consists in universal HIV testing to enhance the identification of all HIV-positive individuals followed by immediate treatment of all HIV-positive individuals, irrespective of their CD4 cell counts.UTT is a global public health approach at hart and should neither be compulsory nor coercive. It is broadly accepted that it would not be easily achievable but it could provide a framework to enhance existing interventions, for instance, TLC+ is a study to assess the feasibility of a community-level test, link to care, plus treat strategy in the United States.
AVAC provides a lay introduction to the Test and Treat approach and a summary table of a number of planned and ongoing feasibility studies of the approach. Numbers in bracket refer to peer-review articles which can be downloaded here. |


“A key premise of the Test and Treat approach is that everybody should first be able to test for HIV.”
Quite so. I asked Reuben Granich what would it take to ensure that everybody was able to test for HIV, perhaps once a year (the premise requires that they be able to test regularly), in a country like Kenya. He said he couldn’t answer the question. That was in 2008, just after he published the paper. I wonder if he is any closer to answering it now.